
Many general dental offices in the U.S. operate with fewer than 10 employees, exempting them under OSHA’s recordkeeping rules (29 CFR §1904) from maintaining injury and illness logs. At the same time, dental employees are routinely exposed to mercury through the placement, polishing, and especially during the removal of dental mercury amalgam fillings. OSHA considers Mercury to be a highly toxic chemical hazard, which is an established neurotoxin with well-documented occupational risks, including neurotoxicity and reproductive harm.
This creates a clear circular logic flaw:
Despite widespread use of mercury within dentistry, OSHA classifies dental practices as a low-hazard industry (NAICS code 621210, Offices of Dentists) based on Bureau of Labor Statistics (BLS) data showing low reported Days Away, Restricted, or Transferred (DART) rates below the private-sector average.
However, the vast majority of dental offices have fewer than 10 employees and fall into this low-hazard category. As a result, they are not required to routinely track or report injuries and illnesses. This absence of data then reinforces and perpetuates the “low-hazard” designation.
Why Chronic, Low-Level Mercury Exposure Remains Invisible in Official Statistics
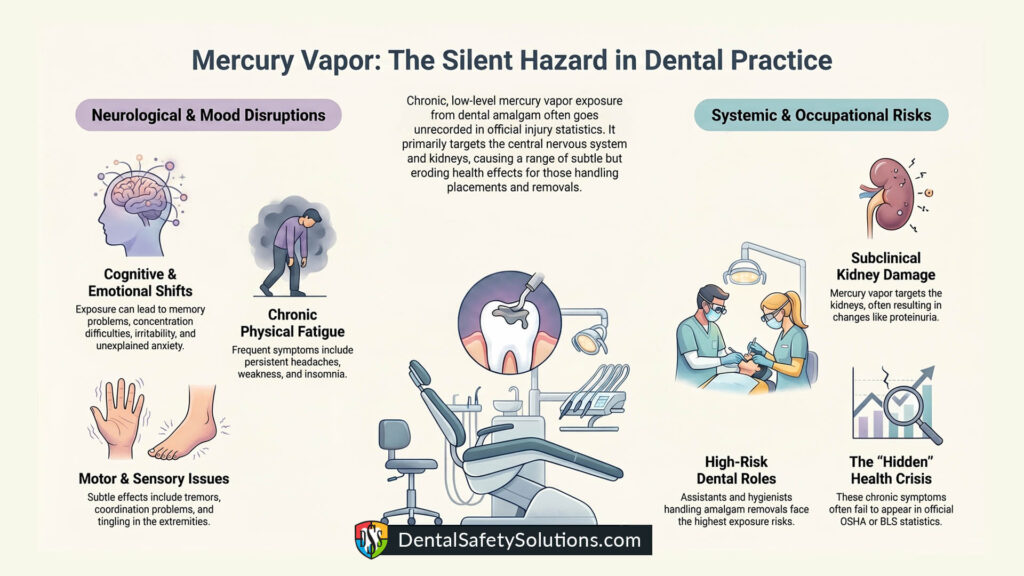
Chronic, low-level mercury vapor exposure from dental amalgam can quietly erode the health of dental employees—especially assistants and hygienists who frequently handle removals and placements—without appearing clearly in OSHA or BLS injury and illness statistics.
Elemental mercury vapor primarily targets the central nervous system and kidneys. Subtle, chronic effects often include:
- Tremors, headaches, fatigue, weakness, and insomnia
- Mood changes (irritability, anxiety, depression, excessive shyness)
- Cognitive issues (memory problems, concentration difficulties)
- Neuromuscular effects (tingling, coordination problems)
- Subclinical kidney changes (such as proteinuria)
These symptoms are non-specific and overlap heavily with common conditions like stress, burnout, aging, migraines, depression, or fibromyalgia. Physicians rarely suspect occupational mercury toxicity in a dental worker unless there is an obvious acute exposure incident.
BLS and OSHA data focus on acute, reportable events. The DART rates that classify dental offices as “low-hazard” track observable injuries and acute illnesses that result in lost work time or job restrictions. They do not effectively capture:
- Slow-building chronic neurotoxicity
- Subclinical effects that reduce quality of life or productivity without causing formal “days away”
- Conditions misdiagnosed as unrelated to work (e.g., “just anxiety” or “normal aging”)
Serious chronic effects would require clear medical documentation linking them to occupational exposure—something that is rare without targeted testing (such as urine mercury levels, especially post-chelation provocation, or specialized neurological evaluation).
Multiple studies of dental personnel have found higher rates of neurological symptoms, memory and concentration difficulties, mood disturbances, and subtle motor or cognitive deficits that correlate with mercury body burden—even at relatively low modern exposure levels. Dental staff show higher urine mercury levels than the general population. Pre-1990s exposures were substantially higher due to less advanced ventilation, non-encapsulated amalgam, and fewer engineering controls.
When employees are not properly informed about mercury risks (or when they downplay vague symptoms), they often fail to connect their health issues to work or request targeted testing.
This creates a self-reinforcing feedback loop: low reported injuries and illnesses → low-hazard classification → reduced regulatory scrutiny → continued under-recognition of chronic chemical hazards.
Individual susceptibility varies due to genetics, nutrition, co-exposures, and other factors, so effects are not uniform across workers. Nevertheless, the current system is heavily biased toward visible, acute harms. Insidious, cumulative toxins like mercury vapor can degrade long-term health in ways that official statistics systematically miss—making the “low-hazard” label for dental offices potentially misleading when it comes to chronic occupational chemical exposure.
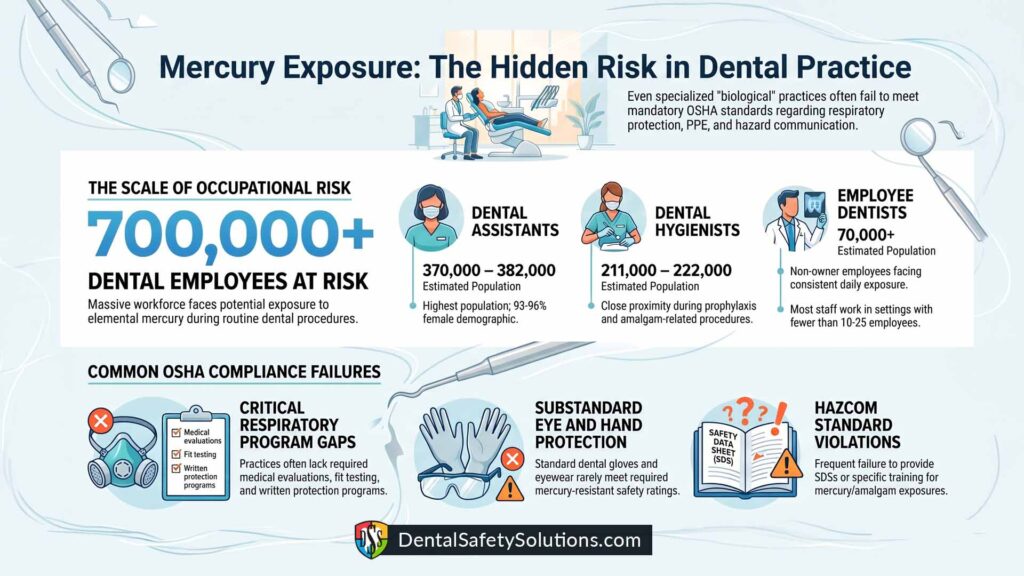
Magnitude of the Problem: Dental Employees at Risk
– Dental Assistants: Approximately 370,000–382,000, with 93–96% female.
– Dental Hygienists: Approximately 211,000–222,000, with 94–98% female. Hygienists routinely work in close proximity during prophylaxis, polishing, and amalgam-related procedures.
– Employee Dentists: An estimated 70,000+ non-owner employees, ~48.3% female.
Combined, well over 650,000–700,000 dental employees face potential occupational exposure to elemental mercury.
DSO vs. Small Practice Employment
A growing share of dental professionals (16–30%+ of dentists) work in Dental Service Organizations (DSOs). Larger DSOs (many with well over 25 employees at the enterprise or site level) employ tens of thousands of assistants and hygienists. However, the majority of dental staff still work in smaller independent or small-group practices that fall under the 10- or 25-employee thresholds for reduced recordkeeping and penalty relief.
Comparison: Two Biological Dental Offices Failing OSHA Requirements
Both offices are biological dental practices that explicitly recognize the serious health threats posed by mercury vapor and particulate generated during amalgam removal. They equip employees with respirators during these procedures. Nevertheless, they fail to comply with multiple formal OSHA requirements.
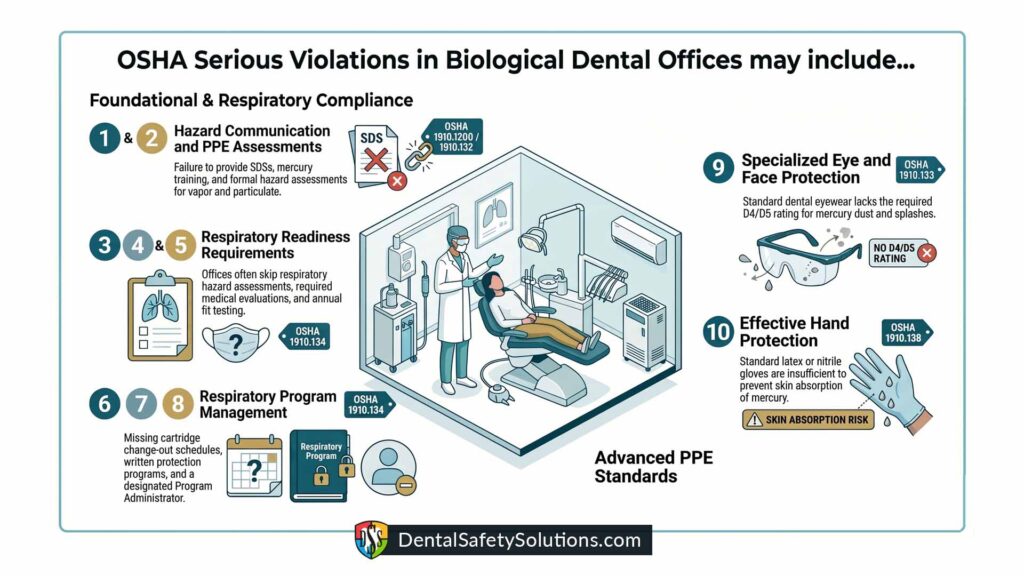
These offices commit the following serious violations:
Respiratory Protection Standard (1910.134)
– No hazard assessment for respiratory hazards [1910.134(d)(1)(iii)]
– No medical evaluations before respirator use [1910.134(c)(1)(ii)]
– No fit testing [1910.134(c)(1)(iii)]
– No cartridge change-out schedule [1910.134(d)(3)(iii)(B)(2)]
– No written respiratory protection program [1910.134(c)]
– No designated Respiratory Program Administrator [1910.134(c)(3)]
Hazard Communication Standard (1910.1200)
– Failure to provide SDSs, employee training, and a written HazCom program for mercury/amalgam exposures.
Eye and Face Protection (1910.133)
– Failure to provide appropriate eye and face protection. Standard dental eyewear is generally not rated D4 or D5 (for dust, impact, and splash). Amalgam removal generates both vapor and particulate that can contact the eyes and face. Proper ANSI Z87.1-rated safety eyewear (D4/D5) and/or faceshields are required.
Hand Protection (1910.138)
– Failure to provide appropriate hand protection. Standard dental gloves (latex or nitrile) are not rated or sufficient to protect against skin absorption of elemental mercury.
General Requirements – Personal Protective Equipment (1910.132(a))
– Failure to perform a hazard assessment to identify and evaluate workplace hazards (including respiratory, eye/face, and skin hazards from mercury vapor and particulate) and to select appropriate PPE.
OSHA’s July 2025 Penalty Reduction Policy
In July 2025, OSHA expanded significant penalty reductions for small employers. A 70% size-based reduction (previously limited to 10 or fewer employees) now applies to employers with up to 25 employees. Additional discounts include 15% for immediate corrective action (quick-fix) and 20% for employers with no inspection history or no prior serious violations. These reductions can compound dramatically. While intended to help small businesses, the policy further reduces financial incentives for rigorous hazard control in the many dental offices that fall under these thresholds.
Key Effects of “Serious” Classification on Penalties
Serious violations typically start at or near the full gravity-based penalty of $16,550 (especially high-gravity ones with greater probability of serious harm). Reductions for size (up to 70% for employers with ≤25 employees), history (20% for a clean record), and good faith (up to 25%) remain fully available. However, the 15% quick-fix reduction generally does not apply to high-gravity serious violations—it is available only for low- or moderate-gravity serious violations. Serious violations also have a policy minimum penalty floor (around $1,221 after all applicable reductions in recent years) and will not drop to $0. Reductions are discretionary; the Area Director can withhold or limit them for deterrent purposes (e.g., multiple serious violations or perceived lack of cooperation). The typical order of application is size → history/good faith → quick-fix (if eligible).
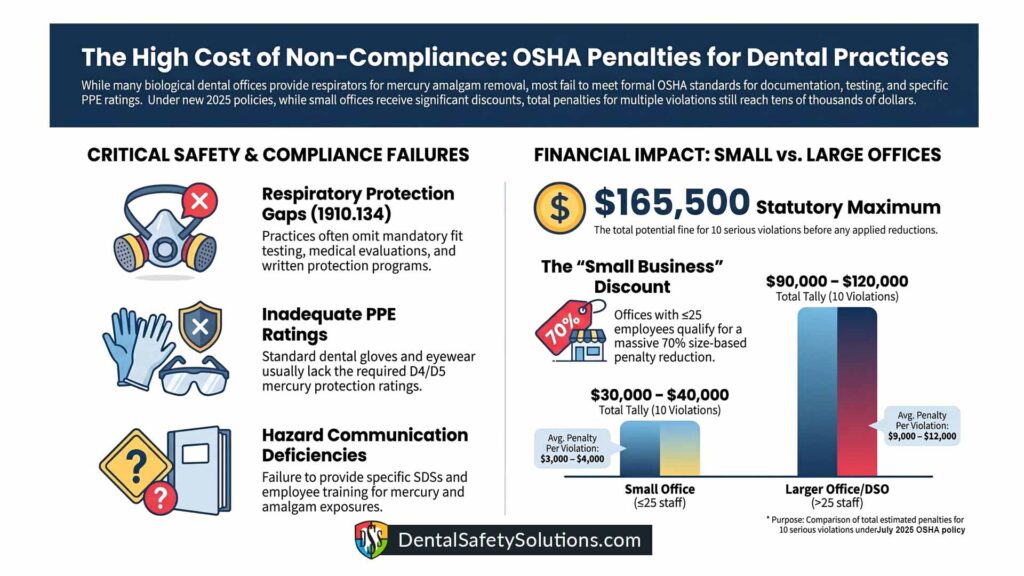
Without any reductions (full statutory penalties):
10 violations × $16,550 = $165,500 total for either office.
Small Office (<25 employees) — Assuming moderate- or low-gravity serious violations and full eligibility for all reductions: 70% size reduction → $16,550 × 0.30 = $4,965 20% history reduction → $4,965 × 0.80 = $3,972 15% quick-fix (if eligible) → $3,972 × 0.85 ≈ $3,376 per violation. Realistic final range per violation: Roughly $3,000–$4,000 (or down to the ~$1,221 minimum). Without the quick-fix step (high-gravity), it would be around $3,972. Tally for 10 violations: $30,000 – $40,000 total (or lower with maximum discretion and good-faith application).
Larger Office/DSO Site (>25 employees):
Receives only 0–30% size reduction. Quick-fix is more likely to apply if gravity is moderate/low, but overall relief is significantly less.
Realistic final range: Roughly $9,000–$12,000 per violation.
Tally for 10 violations: $90,000 – $120,000 total (roughly 2.8–3.5 times higher than the small office for identical violations).
Even with substantial reductions available to small employers, the proposed fines for these serious violations can still reach tens of thousands of dollars. Larger operations face meaningfully higher financial exposure.
Mercury Monitoring and Medical Surveillance
Unlike other heavy metals such as lead, OSHA has no substance-specific mercury standard requiring routine monitoring or medical surveillance. Mercury (elemental, inorganic, and organic forms) lacks a dedicated OSHA standard like lead’s. It falls under the general industry air contaminants standard (29 CFR 1910.1000, Table Z-2):
Permissible Exposure Limit (PEL): Generally 0.1 mg/m³ (100 µg/m³) as an 8-hour TWA for mercury vapor (with a ceiling of 0.1 mg/m³ in some contexts). Lower recommendations exist from NIOSH (0.05 mg/m³) and ACGIH (0.025 mg/m³), but these are not enforceable by federal OSHA.
There is no mandatory routine air monitoring or action level that automatically triggers ongoing sampling. Additionally, there is no required medical surveillance or biological monitoring (e.g., urine or blood mercury testing) mandated by a substance-specific rule. Employers must still comply with the general duty clause (Section 5(a)(1) of the OSH Act) to provide a workplace free from recognized hazards, and the Hazard Communication standard (1910.1200) for training and labeling.
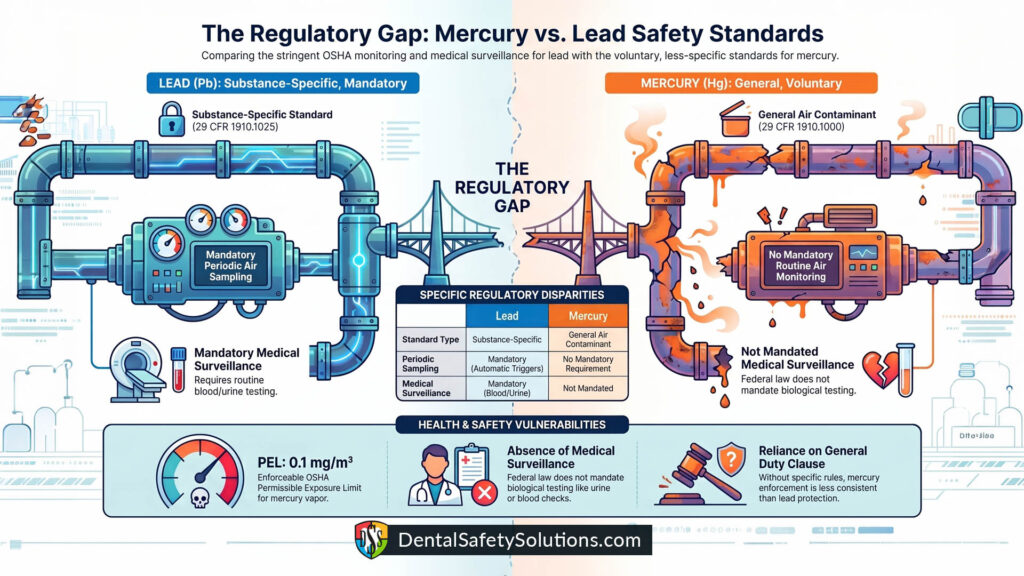
In practice, responsible employers should conduct voluntary air monitoring, biological testing, and medical surveillance for mercury (especially in industries like dental, chlor-alkali plants, or recycling), following NIOSH or ACGIH guidance. However, unlike lead, these are not federally mandated unless site-specific conditions (e.g., HAZWOPER operations) bring in other rules. Why the Difference? Lead has a long history of well-documented occupational poisoning with clear dose-response data, leading to the 1978 standard.
Mercury regulation is more fragmented (different PELs for vapor vs. compounds). OSHA has not updated it with a comprehensive substance-specific rule, even though mercury is highly neurotoxic and can be absorbed through skin and inhalation. This gap means enforcement for mercury relies more on general standards, which can result in less consistent protection compared to lead.
Employers have more flexibility (and responsibility) to assess risks themselves, whereas lead triggers automatic compliance programs once exposure thresholds are met. Many safety professionals recommend treating mercury with similar vigilance to lead, especially given modern lower safety limits.
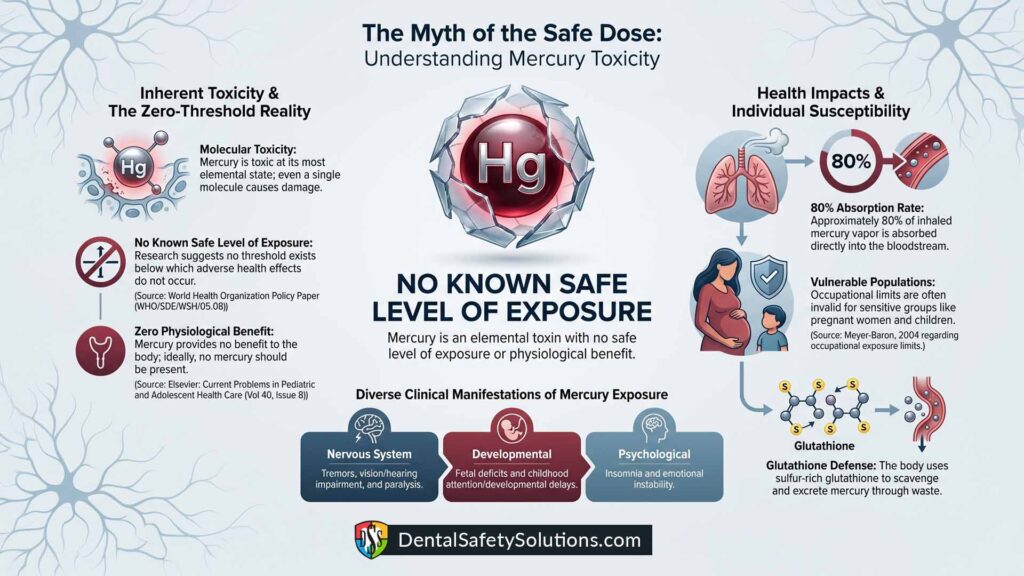
No Safe Level of Mercury
Furthermore, leading health authorities have concluded there is no known safe level of mercury exposure. The World Health Organization has stated that recent studies suggest mercury may have no threshold below which some adverse effects do not occur. Research on children’s health has similarly concluded there is no known safe level of exposure and that ideally neither children nor adults should have any mercury in their bodies because it provides no physiological benefit. This is especially relevant for dental workers. Studies have shown that dentists and dental assistants are exposed to higher mercury concentrations than the general population. Importantly, current occupational exposure limits are not considered valid when discussing sensitive or vulnerable individuals, including pregnant women and children. Some people are particularly sensitive to mercury toxicity due to genetic polymorphisms, and there is insufficient dose-response data for immunologically vulnerable persons. As a result, no zero-effect level can be established where mercury-related symptoms do not occur.
Conclusion: Persistent Regulatory Gaps and the Need for Stronger Protections
The current regulatory framework creates a self-reinforcing cycle in which dental offices are labeled low-hazard largely because chronic, low-level mercury exposures and their subtle neurological effects are systematically underreported and poorly captured by existing surveillance systems. With no known safe level of mercury exposure and occupational limits that fail to adequately protect vulnerable individuals, the reliance on an outdated PEL, combined with broad exemptions from recordkeeping and generous penalty reductions for small employers, leaves hundreds of thousands of dental workers—particularly assistants and hygienists—exposed to preventable harm.
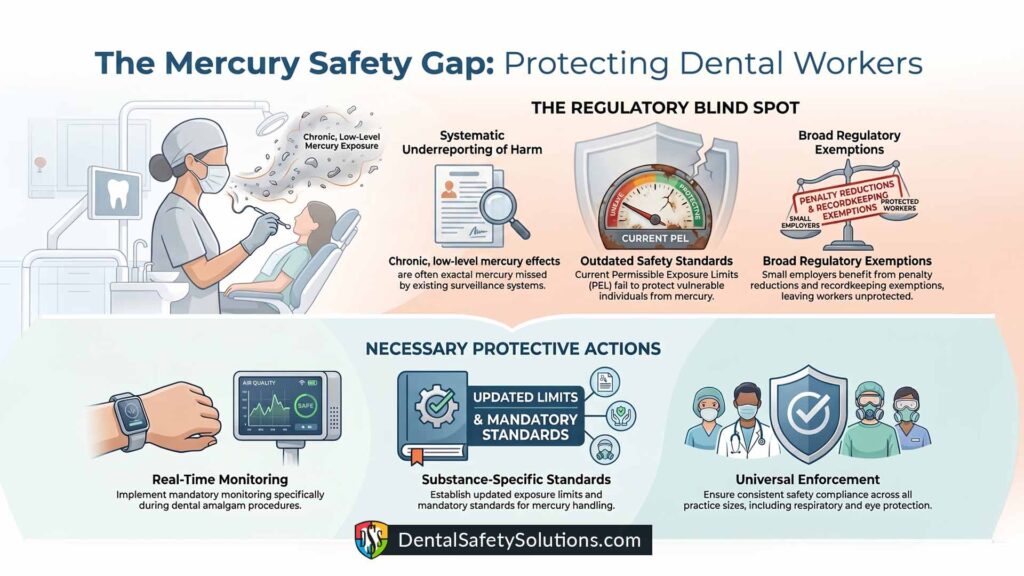
Even biological dental practices that recognize mercury’s dangers often fall short of full OSHA compliance in respiratory protection, hazard communication, eye and face protection, and hand protection.
Without updated exposure limits, mandatory substance-specific standards, real-time monitoring during amalgam procedures, and consistent enforcement across all practice sizes, the gap between recognized risk and actual worker protection will persist. Stronger regulatory action is needed to close these blind spots and ensure that dental workers are not left to bear the hidden costs of an outdated system.
Simple Solutions
Breaking free from the cycle of circular thinking around OSHA penalties and compliance doesn’t have to be complicated or overwhelming. By partnering with Dental Safety Solutions, your practice can designate and fully prepare one of your own employees to serve as the Respiratory Program Administrator through our comprehensive certification course.

This includes required OSHA documentation customized for your practice, essential equipment such as fit-test kits and mercury wipes, and ongoing support to ensure full compliance with OSHA 1910.134. We also offer a 10% discount to members of the International Academy of Biological Dentistry & Medicine.
If no one on staff is available or willing to take on the role, your practice can simply hire one of our already-certified Respiratory Program Administrators who have successfully completed the course. Either path safeguards your team’s health, reduces liability, and builds a stronger culture of safety. Visit Dental Safety Solutions today to explore pricing options tailored to your team size and take confident control of your compliance future.